
In clinical practice, this condition is treated by opening the chest by median sternotomy or thoracotomy with cardiopulmonary bypass. The cardiac surgeons of the Department of Cardiovascular Surgery at Almazov Centre successfully performed the procedure using endoscopic access through centimeter incisions in the chest without cardiopulmonary bypass. This innovative treatment approach has not been previously described in the scientific literature.
A 52-year-old female patient presented to Almazov Centre seeking medical help. She had been experiencing an irregular heartbeat for approximately three years, accompanied by dizziness, weakness, and decreased blood pressure. Upon examination in the hospital, additional diagnostic procedures (transesophageal echocardiography and multispiral CT of the heart) revealed an aneurysmal dilatation of the left atrial appendage measuring 70*55*45 mm.
Left atrial appendage aneurysm is a rare cardiac anomaly that is usually incidentally found in middle-aged patients. Though initially asymptomatic, it is a dangerous condition directly predisposing to atrial arrhythmias. In this case, surgery is indicated in order to prevent the development of complications associated with ischemic stroke.
The surgical team, led by cardiovascular surgeon Dr. Arthur Bagdasaryan, considered the anatomical characteristics of the aneurysm (presence of the neck) and decided to perform minimally invasive endoscopic resection of the aneurysm and radiofrequency ablation in the left atrium without cardiopulmonary bypass to treat arrhythmia attacks (atrial fibrillation).

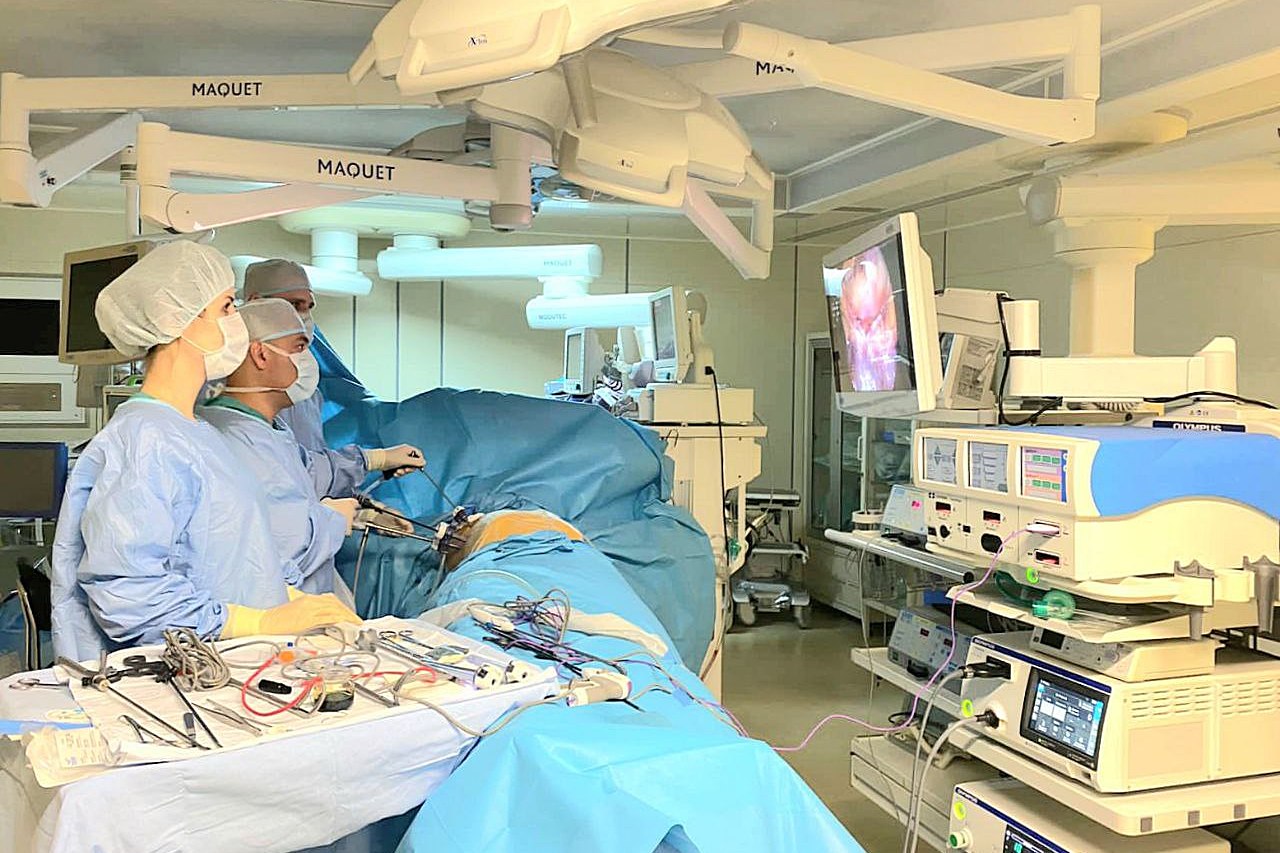
From left to right: Timofey Scherbinin, cardiovascular surgeon; Artur Bagdasaryan, cardiovascular surgeon; Alexander Gnevashev, Head of Cardiovascular Surgery Department 1; Arzuv Agamamedova, clinical resident in cardiovascular surgery
Once the pericardium on the left side had been opened, a large aneurysm originating from the left atrial appendage was identified. The aneurysm was then clamped and fixed using transesophageal echocardiography, with an additional vascular clamp, sutured and resected with a special suturing device along its basis. Finally, a combined radiofrequency ablation procedure was performed.
The postoperative period was uneventful. No rhythm disturbances were observed. The patient was discharged from the surgical department on the seventh postoperative day.